
Rheumatoid arthritis (RA) is a systemic, debilitating, chronic inflammatory autoimmune disorder affecting approximately 1% of the world population (1). The disease severely impacts quality of life with increased morbidity and reduced life expectancy.
 With undefined pathogenesis, different studies report a blend of environmental and genetic factors responsible for full expression of the disease. The shared epitopes coded by human leukocyte antigen (HLA) alleles, non-HLA genes, epigenetic factors, and differentially glycosylated proteins are considered significant risk factors for progression of RA (2-3). Elevated levels of rheumatoid factors (RF) (4), anti-cyclic citrullinated peptide autoantibodies (5) and anti-mannose-binding lectin autoantibodies are some examples of autoimmune responses by RA patients. These factors, however, contribute approximately 50% to the risk of development of RA while the rest may be contributed by host–environment interactions (6). Environmental factors responsible for development of RA may present and act even before disease symptoms become apparent. Early environmental factors such as high birth weight promotes chances of development of RA and early start of breast feeding reduces chances of development of RA (7). Other environmental factors such as smoking and infectious diseases also pose risk of developing RA (8)
With undefined pathogenesis, different studies report a blend of environmental and genetic factors responsible for full expression of the disease. The shared epitopes coded by human leukocyte antigen (HLA) alleles, non-HLA genes, epigenetic factors, and differentially glycosylated proteins are considered significant risk factors for progression of RA (2-3). Elevated levels of rheumatoid factors (RF) (4), anti-cyclic citrullinated peptide autoantibodies (5) and anti-mannose-binding lectin autoantibodies are some examples of autoimmune responses by RA patients. These factors, however, contribute approximately 50% to the risk of development of RA while the rest may be contributed by host–environment interactions (6). Environmental factors responsible for development of RA may present and act even before disease symptoms become apparent. Early environmental factors such as high birth weight promotes chances of development of RA and early start of breast feeding reduces chances of development of RA (7). Other environmental factors such as smoking and infectious diseases also pose risk of developing RA (8)
 Early recognition and treatment of RA is complicated because of heterogeneous nature of the disease. No biomarker is available to detect the early onset of disease, and traditional biomarkers may not identify all patients that require early therapeutic interventions (9), and thus, the patients face severe complications with serious joint damage and disability. The first line of treatment for RA includes disease-modifying antirheumatic drugs (DMARDs) that suppress disease activity and reduce joint damages. Continuous administration of biologics being the only option for prolonged remission, however, this being expensive is still beyond the reach of most people in the urban and the rural sectors.
Early recognition and treatment of RA is complicated because of heterogeneous nature of the disease. No biomarker is available to detect the early onset of disease, and traditional biomarkers may not identify all patients that require early therapeutic interventions (9), and thus, the patients face severe complications with serious joint damage and disability. The first line of treatment for RA includes disease-modifying antirheumatic drugs (DMARDs) that suppress disease activity and reduce joint damages. Continuous administration of biologics being the only option for prolonged remission, however, this being expensive is still beyond the reach of most people in the urban and the rural sectors.
Furthermore, patients with RA generally complain of gastrointestinal tract problems particularly dyspepsia (bloating, postprandial fullness, nausea, early satiety, epigastric pain, and burning and belching), mucosal ulceration, and altered bowel habits (constipation/diarrhea) (10). Recently, Littman laboratory identified Prevotella copri significantly prevalent in RA patients than healthy controls providing the support that the “gut-joint axis” hypothesis is relevant for human rheumatic diseases and may lead to pathogenesis of RA (11).
Dietary Interventions in RA
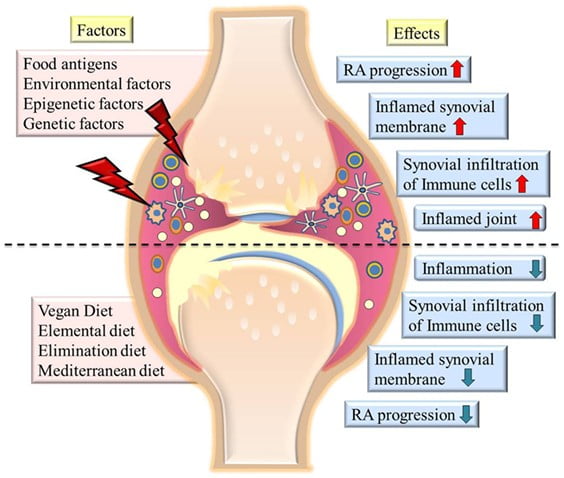
With the increasing evidence of altered microbiota in the gut of RA patients being responsible for pathogenesis as well as disease progression (12,13,14, it should be desirable for rheumatologists to advocate a supplemental “diet therapy” to RA patients. Various dietary plans for RA have been reported since longand are being repeatedly projected), such as medically supervised 7–10 days fasting ), vegan or Mediterranean diets (MDs)
Nutritional epidemiology has seen a shift away from single nutrient analyses to a complementary approach in the form of dietary pattern analysis (). Evaluating dietary patterns can provide a more holistic and clinically relevant approach to assessing diet-disease relations as nutrients are not eaten in isolation and synergistic effects of multiple components can have a concerted effect (15). Vegetarian-based dietary patterns are typically higher in fruits, vegetables, whole grains, nuts, seeds, and legumes, all of which are naturally higher in phytochemicals and some vitamins compared to non-vegetarian dietary patterns . A variety of vegetarian-based eating patterns exist based on the inclusion or exclusion of animal products. For example, individuals who omit all animal products are classically described as vegan, whilst those who include eggs and dairy products are referred to as lacto-ovo-vegetarian (LOV) . Consumption of these dietary patterns are protective against many chronic diseases, including coronary heart disease, type 2 diabetes mellitus (T2DM), some cancers, and are associated with lower all-cause mortality.
References
1. Gibofsky A. Overview of epidemiology, pathophysiology, and diagnosis of rheumatoid arthritis. Am J Manag Care (2012) 18(13 Suppl):S295–302.
2.Holoshitz J. The rheumatoid arthritis HLA-DRB1 shared epitope. Curr Opin Rheumatol (2010) 22(3):293. doi:10.1097/BOR.0b013e328336ba63
3. Rioux JD, Abbas AK. Paths to understanding the genetic basis of autoimmune disease. Nature (2005) 435(7042):584–9. doi:10.1038/nature03723
4. Eggert M, Zettl U, Neeck G. Autoantibodies in autoimmune diseases. Curr Pharm Des (2010) 16(14):1634–43. doi:10.2174/138161210791164144
5. Rantapää-Dahlqvist S, de Jong BA, Berglin E, Hallmans G, Wadell G, Stenlund H, et al. Antibodies against cyclic citrullinated peptide and IgA rheumatoid factor predict the development of rheumatoid arthritis. Arthritis Rheum (2003) 48(10):2741–9. doi:10.1002/art.11223
6 Edwards CJ. Commensal gut bacteria and the etiopathogenesis of rheumatoid arthritis. J Rheumatol (2008) 35(8):1477–9.
7. Jacobsson LT, Jacobsson ME, Askling J, Knowler WC. Perinatal characteristics and risk of rheumatoid arthritis. BMJ (2003) 326(7398):1068–9. doi:10.1136/bmj.326.7398.1068
8.Edwards C, Cooper C. Early environmental factors and rheumatoid arthritis. Clin Exp Immunol (2006) 143(1):1–5. doi:10.1111/j.1365-2249.2005.02940.x
9.Gonzalez-Alvaro I, Ortiz AM, Seoane I, García-Vicuña R, Martínez C, Gomariz R. Biomarkers predicting a need for intensive treatment in patients with early arthritis. Curr Pharm Des (2015) 21(2):170–81. doi:10.2174/1381612820666140825123104
10. Wolfe F, Kong SX, Watson DJ. Gastrointestinal symptoms and health related quality of life in patients with arthritis. J Rheumatol (2000) 27(6):1373–8.
11.Scher JU, Sczesnak A, Longman RS, Segata N, Ubeda C, Bielski C, et al. Expansion of intestinal Prevotella copri correlates with enhanced susceptibility to arthritis. Elife (2013) 2:e01202. doi:10.7554/eLife.01202
12Vaahtovuo J, Munukka E, Korkeamäki M, Luukkainen R, Toivanen P. Fecal microbiota in early rheumatoid arthritis. J Rheumatol (2008) 35(8):1500–5.
13. Toivanen P. Normal intestinal microbiota in the aetiopathogenesis of rheumatoid arthritis. Ann Rheum Dis (2003) 62(9):807–11. doi:10.1136/ard.62.9.807
14. Scher JU, Sczesnak A, Longman RS, Segata N, Ubeda C, Bielski C, et al. Expansion of intestinal Prevotella copri correlates with enhanced susceptibility to arthritis. Elife (2013) 2:e01202. doi:10.7554/eLife.01202
15 Jacobs DR Jr, Gross MD, Tapsell LC. Food synergy: an operational concept for understanding nutrition. Am J Clin Nutr. 2009;89(5):1543S–8S. [PMC free article] [PubMed] [Google Scholar]

Madelena has been my nutritionist since February, and I feel extremely grateful to have met her. She is a kind, welcoming and has vast knowledge about her work.
For many years I have suffered with medical issues. one of my biggest challenges I was having was with my feet and not being able to walk properly as I was always in constant pain.
Doctors where only able to prescribe an assortment of medication which only masked the pain and led to more issues.
From meeting Madelena, she was able to regularise my eating habits, advise me on what and when to eat and certain supplements and vitamins to take.
At first it was very difficult to stop eating the foods I’ve enjoyed for most of my life, but once again, she was understanding of this and worked with me to cut them down and help me overcome this.
Within a month I could feel the difference this was having on me. Movement was becoming more easier; my weight gain was reduced, and my overall well-being was improved. Although, I still take medication at present, it is dramatically decreased making the associated issues I was experiencing from the medication cease.
I am so grateful to Madeleina as she has given me back hope.
If you are thinking about using her services, I totally recommend her